
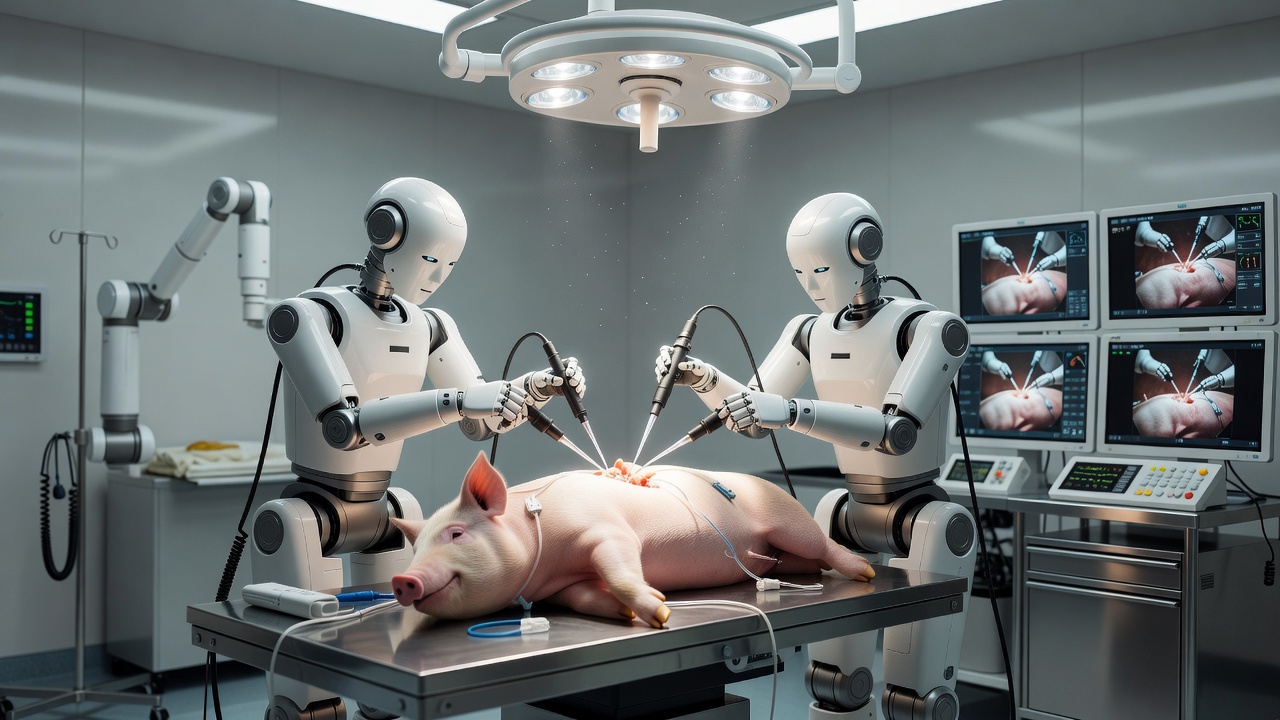
Surgeons at the University of California San Diego have achieved what no one had before. They guided two teleoperated humanoid robots through successful gallbladder removals on live pigs. The procedures mark the first time such machines completed surgeries on living subjects under remote human direction.
The robots, known as Surgie, stand just five feet tall and weigh 60 pounds each. Their compact size sets them apart from bulky conventional systems that can tip the scales at 1,800 pounds and demand dedicated operating room space. Engineers adapted off-the-shelf Unitree G1 models, which start at about $13,500, to grip standard laparoscopic tools through custom adapters and software.
One operation paired a humanoid with a human assistant. The other relied entirely on two robots working in tandem. Both pigs came through the minimally invasive cholecystectomies without complication. Yet the sessions ran longer than typical because operators paused repeatedly to recalibrate the systems and manage latency that sometimes stretched into hundreds of milliseconds.
Still, the precision matched what surgeons expect from established teleoperated platforms. “We were surprised at how well Surgie meshed with our workspace and workflow,” said Nikita Thareja, a general surgery resident at UC San Diego. The remark, reported by UC San Diego Today, captured the team’s cautious optimism after months of preparation at the university’s Center for the Future of Surgery.
Michael Yip, professor in the Department of Electrical and Computer Engineering and senior author on the study, sees broader possibilities. “Remotely operated and autonomous humanoid robots have real potential for amplifying access to critical surgeries to which patients would otherwise not have access,” he told the same outlet. “This can help address the healthcare crisis not only in the United States, but also worldwide.”
The project, published in Nature, builds on years of incremental progress in surgical robotics. Previous autonomous systems from Johns Hopkins had stitched pig intestines or removed gallbladders from cadavers without real-time human input. Those efforts, detailed in Johns Hopkins Hub, focused on machine learning and computer vision rather than direct teleoperation.
But the UC San Diego approach takes a different path. It uses human skill at the controls while the humanoid form factor promises versatility that rigid, multi-arm da Vinci systems cannot match. A surgeon in one city could direct a robot in another. Or in a battlefield tent. Or aboard a spacecraft. “It’s a fraction of the cost and it takes a fraction of the space in an operating room,” explained Shanglei Liu, an assistant professor of surgery. “So it’s easy to deploy, anywhere from rural areas, to the battlefield, and even to space.” His comments appeared in the UC San Diego release.
Latency remains a stubborn obstacle. Current delays exceed the 150-millisecond threshold many experts consider ideal for fluid control. The robots’ 450-millimeter arm span also limits reach compared with human anatomy. Engineers addressed these constraints during the trials by inserting recalibration breaks. Future iterations will need faster networks, better motion mapping, and perhaps onboard sensors that anticipate surgeon intent.
Cost advantages could prove decisive. The da Vinci Surgical System often exceeds $500,000 before maintenance contracts and disposables drive annual expenses into the millions. Smaller hospitals and clinics have largely stayed away. Humanoids that roll into any standard operating room and use existing instruments could change that equation. They might even tidy the room or retrieve supplies between steps. Early tests suggest such multitasking lies within reach.
Ryan Broderick, interim director of the Center for the Future of Surgery, praised the cross-disciplinary effort. “This achievement reflects the power of bringing engineers and surgeon innovators together to solve meaningful clinical problems at our world-class training and research lab,” he said, according to UC San Diego Today. The team included engineers Lucas Zekai Liang, Peihan Zhang, Calvin Joyce, Soofiyan Atar and Florian Richter alongside surgeons Garth Jacobsen and others.
Recent coverage has placed the accomplishment in context. Ars Technica noted the preclinical nature of the work and the robots’ origins as relatively affordable consumer-grade hardware. The story highlighted how the setup translates human movements from a console, stereo headset and foot pedals into robot actions. It also flagged the same technical shortcomings the UCSD researchers openly discussed.
Interest on X has been brisk though largely anecdotal. Users shared the UCSD video demonstration, which shows the robots maneuvering trocars and dissecting tissue with careful, if sometimes hesitant, motions. Some posts drew parallels to earlier autonomous feats. Others wondered aloud about liability when a robot eventually operates without constant human oversight.
Yip and his colleagues already outline the next phase. They aim to evolve these platforms into autonomous surgical assistants that handle routine tasks while humans focus on complex decision-making. “One of our goals is to develop the autonomous surgical assistant,” Yip stated. “Our goal is an operating theatre of the future, where humanoid robots and humans work side by side as an integrated team to deliver procedures to those in need, both in traditional hospital settings as well as in non-traditional, field medicine scenarios.”
The distinction between teleoperated and fully autonomous systems matters. The former keeps expert judgment in the loop. The latter promises scalability but introduces questions around safety, regulation and training. Chinese researchers reported an AI-driven robot completing biliary surgery on a pig earlier this year without human intervention, per a South China Morning Post account from January. That work adds to the growing body of evidence that machines can manage soft-tissue procedures.
Yet success on pigs does not guarantee immediate translation to humans. Anatomical differences, regulatory hurdles and the need for thousands of hours of validation stand in the way. The UCSD team performed its operations on large non-primate mammals precisely to approximate human conditions as closely as possible. Even so, the procedures required multiple recalibrations. Refining the technology for clinical use will demand faster response times, more robust error correction and extensive safety protocols.
Surgeon shortages loom large in many regions. Rural hospitals struggle to retain specialists. Conflict zones and disaster areas often lack any surgical capacity. A mobile, low-cost humanoid that an experienced doctor can pilot from afar could narrow those gaps. The same machine might later serve as a skilled assistant in high-volume centers, freeing attending surgeons to oversee multiple rooms.
Challenges extend beyond hardware. Data privacy, cybersecurity and ethical questions about remote responsibility require attention. Who answers if a network outage occurs mid-procedure? How do hospitals credential a surgeon who operates from another continent? These issues will occupy policymakers and professional societies in coming years.
For now the achievement stands as proof of concept. Two humanoid robots, directed by human hands, completed operations that once demanded an on-site specialist. The pigs recovered. The data collected will inform the next generation of systems. And the surgeons and engineers involved say they remain surprised by how naturally the robots fit into the operating room.
That surprise may fade as the technology matures. What once seemed like science fiction now looks like an incremental, practical step toward wider surgical access. The road from preclinical success to routine clinical adoption is long. But the first footprints on that road were left this month by a pair of five-foot-tall machines and the doctors who learned to steer them.

