
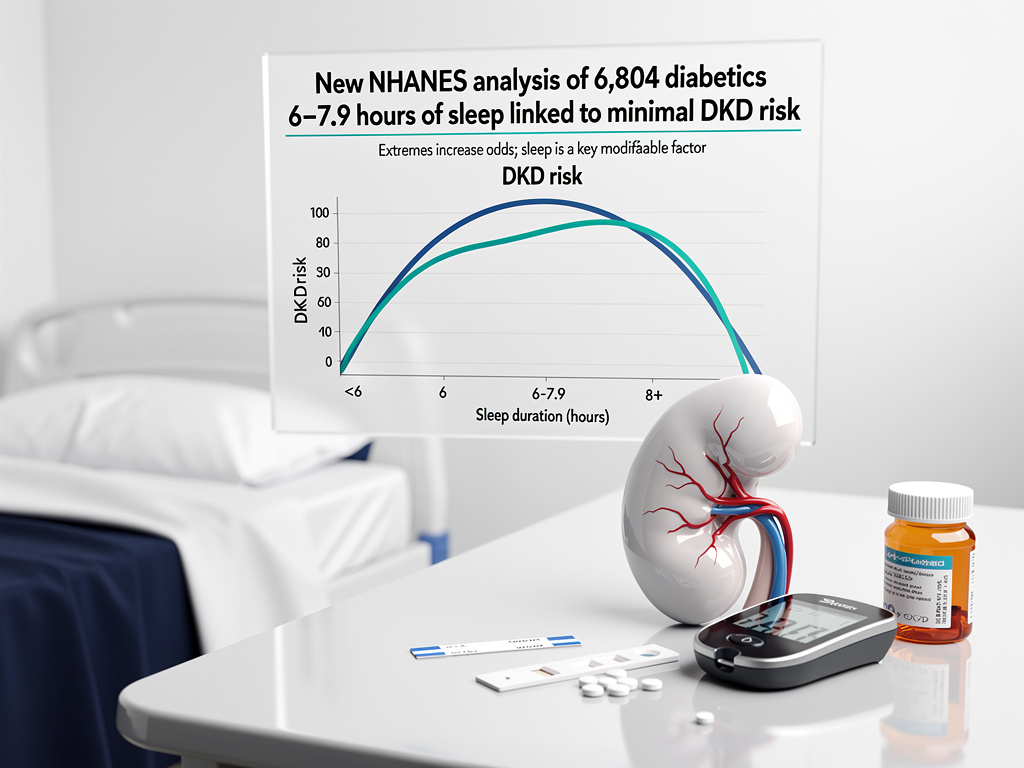
In a finding that underscores sleep as a modifiable pillar of diabetes care, researchers have pinpointed 6.0 to 7.9 hours of nightly rest as the range linked to the lowest risk of diabetic kidney disease, or DKD, among patients with diabetes. This cross-sectional analysis, drawn from 15 years of National Health and Nutrition Examination Survey data, reveals a U-shaped association where deviations—either too little or too much sleep—correlate with heightened DKD odds.
The study, led by Niu D., Zhang L., You Q., and Zhao S., examined 6,804 U.S. adults aged 20 and older with diabetes from NHANES cycles spanning 2005 to 2020. Participants self-reported sleep duration, categorized into quartiles, while DKD was defined through standard clinical markers like reduced estimated glomerular filtration rate or elevated albuminuria. After adjusting for confounders including age, sex, race, BMI, education, marital status, waist circumference, hypertension, smoking, drinking, and coronary artery disease, the 6.0–7.9 hour group emerged with the nadir risk. “Overall, these findings indicate that the lowest risk of diabetic kidney disease is associated with a sleep duration of 6.0–7.9 hours,” the authors noted in Medical Dialogues.
Demographics reflected real-world diabetes burdens: average age 61.1 years, 47.8% female, and 26.0% DKD prevalence. Univariate analyses flagged significant ties between DKD and factors like older age, certain ethnicities, lower education, single status, larger waist circumference, smoking, alcohol use, hypertension, and heart disease—common threads in metabolic syndrome.
Unpacking the U-Curve Risk Pattern
This U-shaped curve aligns with prior research, echoing a 2019 study in Frontiers in Endocrinology on 1,258 Asian diabetics where very short (<5 hours) or long (>8 hours) sleep tied to odds ratios of 2.37 and 2.44 for albuminuria, respectively, versus normal 7-8 hours (ORs from multivariable models adjusted for HbA1c, blood pressure, and more; Frontiers in Endocrinology). Long sleep (>8h) specifically boosted low eGFR risk (OR 2.31, 95% CI 1.27–4.19).
Earlier NHANES work, like Petrov et al.’s 2016 analysis, linked short and long sleep to higher albumin-to-creatinine ratios, hinting at glomerular strain (PubMed). A 2023 cohort in Frontiers in Endocrinology further showed long sleep amplified DKD risk alongside BMI gains, with hazard ratios climbing for extended durations.
These patterns suggest non-linear biology: short sleep spurs inflammation and insulin resistance, eroding glomerular function; excess sleep may signal underlying issues like depression or poor recovery, indirectly taxing kidneys.
Mechanisms at Play in Renal Strain
Sleep governs renal circadian rhythms, influencing sodium excretion, renin-angiotensin activation, and pressure-natriuresis. Disruptions—via short or prolonged durations—elevate sympathetic tone, hypertension, and oxidative stress, accelerating DKD in diabetes-vulnerable kidneys. “The results highlight sleep length as a potentially modifiable aspect of diabetes management,” per the new NHANES paper (Springer).
Supporting evidence from a 2025 prospective cohort found short (≤5h) and long (≥10h) sleep yielded hazard ratios of 1.20 (95% CI 1.04-1.38) and 1.30 (1.09-1.54) for DKD versus 7 hours, mediated partly by obesity markers, inflammation (IL-6, CRP), liver enzymes, and lipids (ScienceDirect). X discussions amplify urgency, with experts like @fmfclips noting one week of 4-6 hour sleep slashes glucose disposal by 50%, mimicking prediabetes.
Diabetes already afflicts 38 million Americans, with DKD striking 30-40%—a leading dialysis trigger. Amid rising obesity and shift work, sleep emerges as a low-cost intervention, potentially easing the $100 billion annual CKD burden.
Cross-Study Echoes and Limitations
Consistency spans datasets: a 2019 NHANES-linked review tied abnormal sleep to reduced eGFR or albuminuria (PMC). Yet cross-sectional designs like Niu’s preclude causality—reverse causation looms, as advanced DKD might disrupt sleep via nocturia or pain.
Self-reported sleep invites recall bias, missing quality metrics like apnea, which confounds 50% of diabetics. Longitudinal gaps persist; a 2025 Brazilian study on weekend catch-up sleep flagged neutral or protective effects against DKD, contrasting weekday shortfalls.
Still, adjusted models robustly isolate sleep’s signal, urging randomized trials on extension interventions.
Clinical Pathways Forward
For clinicians, integrate sleep screening into diabetes visits—target 6-8 hours via hygiene: consistent schedules, dark environments, no screens. Tech like wearables tracks adherence, while CBT-I tackles insomnia outperforming drugs.
Policy eyes workplace reforms; X posts from @EricTopol highlight short sleep’s T2D risk persistence despite diet. As NHANES data evolves, expect refined guidelines, positioning sleep alongside A1c and BP in DKD prevention protocols.
This research reframes diabetes management: not just pills and pumps, but prioritizing rest to safeguard kidneys, the silent victims of metabolic chaos.

