
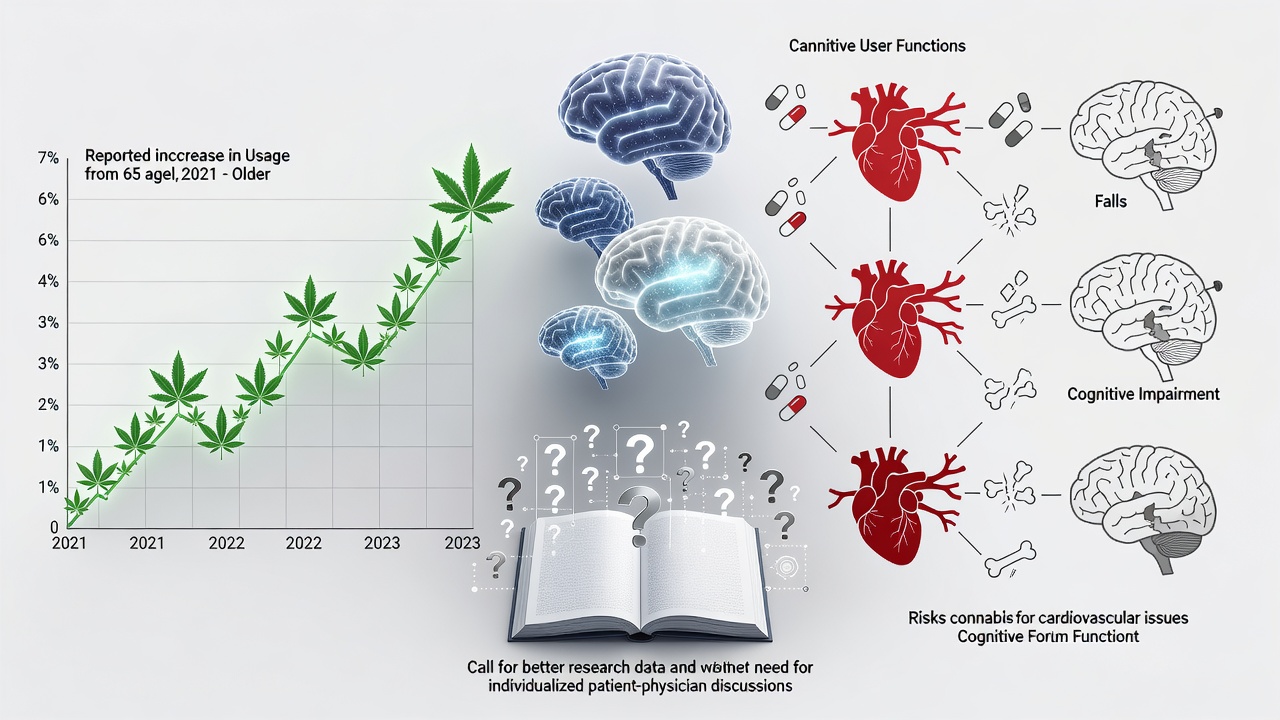
Usage rates among Americans 65 and older jumped nearly 46% between 2021 and 2023. Seven percent now report using cannabis in the past month. JAMA Internal Medicine documented the surge. The numbers reflect a quiet shift. Boomers who once hid their habits now seek relief for pain, sleep troubles and anxiety that come with age.
But does cannabis help or harm? Fresh research offers surprises. Some data point to protective effects on the aging brain. Other findings flag real dangers. Physicians find themselves caught between patient demand and incomplete evidence. The conversation has moved beyond stereotypes. It now centers on data from labs, surveys and clinical observations.
Brain Protection Signals Emerge
Work at the Salk Institute examined cannabinol, a compound produced as THC breaks down. In lab tests on human and animal brain cells, CBN shielded neurons from oxidative stress. The damage this stress causes contributes to diseases like Alzheimer’s. Researchers see potential. Yet they stop short of recommending widespread use. The findings remain preliminary. Futurism reported on the study June 21, 2026.
A separate analysis from CU Anschutz reached even more striking conclusions. Among 26,362 adults ages 40 to 77, greater lifetime cannabis exposure tracked with larger volumes in several brain regions. Cognitive test scores ran higher too. The association held strongest for moderate users. Lead researchers described the pattern as unexpected. They called for more targeted trials. CU Anschutz News published the results in February 2026.
Carl Hart, a Columbia University psychologist, has long pushed back against blanket warnings. His own experiments found no drop in math performance after cannabis use. He points to real-world examples. “Think of all the many people who take cannabis,” Hart told The Washington Post. “There are some people not motivated to do jack, but that isn’t because of cannabis. And there are a wide range of people who have done incredible things in the world while on cannabis. But the notion just won’t die.”
A 2024 study in JAMA Network Open added weight to his view. It tracked middle-aged and older adults who began medical cannabis recently. No significant link to cognitive decline appeared. The adult brain, Hart argues, shows more resilience than alarmist narratives suggest.
Yet other investigations paint a darker picture. Stanford Medicine experts listed heightened risks for those over 65. Heart disease, certain cancers, addiction potential and worsened cognitive issues all appear more likely. Smita Das, a clinical associate professor of psychiatry, noted the lack of consensus on benefits for common complaints like chronic pain or insomnia. “There is no medical consensus that it can help for these conditions,” she said. Stanford Medicine issued the cautions in October 2025.
Canadian health authorities echo the concerns. Adults over 55 process substances differently. Sensitivity rises. Side effects hit harder, especially with existing conditions or multiple medications. Blood pressure fluctuations, dizziness and falls become more probable. Health Canada updated its guidance in April 2026.
Usage patterns tell their own story. A National Poll on Healthy Aging surveyed adults 50 to 80. Eighty-one percent of cannabis users cited relaxation. Sixty-eight percent sought better sleep. Pain relief motivated 63 percent. Mood improvement drew 53 percent. Edibles have gained favor. They avoid smoke and allow precise dosing. Yet potency varies widely. Many products lack clear labeling. Older users sometimes miscalculate intake and experience stronger effects than expected.
Harms show up in the data too. One 2025 study linked cannabis frequency to poor physical and mental health reports. Daily users faced 133% higher odds of 14 or more days of poor mental health in the past month. Physical health complaints rose similarly. Falls, slower walking speed and interactions with prescription drugs add layers of risk. Springer published those associations.
Emergency visits tell another part of the tale. In Canada, cannabis-related ER trips among those 65 and older nearly tripled after legalization. Poisoning cases climbed. Many involved edibles mistaken for ordinary candy. Doctors now see more older patients arriving confused, anxious or with heart symptoms after consumption.
So what explains the surge? Legalization in dozens of states removed legal fears. Cultural acceptance grew. Marketing targeted baby boomers with images of wellness and relief. Higher education and income levels now predict use more than in prior decades. Women’s rates rose sharply. Some credit cannabis with easing menopause symptoms. Others simply prefer it to opioids or sleeping pills.
But evidence for those alternatives remains thin. High-quality randomized trials stay rare. Federal restrictions still complicate research. Scientists rely heavily on observational data and self-reports. Those sources carry bias. Users who feel benefits stay vocal. Those who suffer side effects may stay silent or stop.
Physicians face tough talks. Nathan Stall of the University of Toronto co-wrote an editorial in JAMA Internal Medicine. Therapeutic evidence for medical cannabis in older adults, he noted, looks inconsistent. Possible benefits exist for some conditions. Limited benefit or outright harm appears in others. “The potential harms of cannabis use in older adults are apparent,” Stall and colleagues wrote. They listed cardiovascular events, respiratory problems, sedation, falls and psychiatric issues.
Danielle Haley, assistant professor at Boston University School of Public Health, studied cannabis use disorder. Rates climb fastest among adults 65 and older and those living with HIV. Many face multiple medications. Interactions worry her. “Older adults are an unrecognized group when it comes to cannabis use,” Haley said in May 2025. BU School of Public Health reported her comments. She calls for routine screening and better treatment options for dependence.
Harvard Health took a measured stance. Cannabis may offer safer options than some traditional drugs for certain age-related complaints. Yet it carries harms too. The balance depends on dose, product type, individual health and concurrent medications. Harvard Health laid out the trade-offs in December 2025.
Preclinical hints keep interest alive. Some animal models suggest cannabis compounds might slow aspects of brain aging. Human translation remains uncertain. One UK Biobank analysis found former users sometimes performed better cognitively than never-users. Current heavy use told a different story. Timing appears to matter. Use in adolescence carries documented risks. Midlife and later patterns look more mixed.
Clinicians increasingly recommend honest conversations. Ask about all cannabis forms. Edibles, vapes, topicals and traditional flower each carry distinct profiles. Review medications for interactions. Discuss dosing. Start low. Go slow. Track effects. Some patients report dramatic improvements in quality of life and reduced reliance on other prescriptions. Others experience anxiety, memory lapses or balance problems that outweigh any gains.
Public health officials push for better labeling, age-appropriate warnings and more research funding. Until clearer answers arrive, the message stays cautious. Cannabis is not risk-free for older bodies. Neither is it useless. The truth sits somewhere in the messy middle. Patients and doctors must weigh personal circumstances against the still-evolving science.
And the science continues to arrive. A 2026 review in the American Journal of Preventive Medicine found past-year use at 18.5% for ages 50-64 and 5.9% for those 65 and older. Many consume for medical reasons. Roughly one in five of those users received a formal recommendation. Attitudes have softened dramatically. Most now view medical cannabis as acceptable. Support for restrictions has declined. American Journal of Preventive Medicine captured the shift.
Yet acceptance does not equal endorsement. Experts from Stanford to Toronto agree on one point. More rigorous, longitudinal studies focused on older populations are essential. Current data cannot yet answer basic questions about optimal dosing, long-term brain effects or which patients benefit most. Until those gaps close, physicians will keep offering guidance based on incomplete pictures. Patients will keep experimenting. The gray area persists. So does the need for careful, individualized decisions.

